
A Review of the Works of Neurosurgeon Emil Seletz, MD
Dr. Emil Seletz (b. 1907; d. 1999) was a neurosurgeon in Beverly Hills, California. His publications indicate that he worked at the Los Angeles General Hospital, and he was faculty at the University of California, Los Angeles Medical School. Additionally, his internet biography indicates he was chief of neurosurgery at Cedar’s Hospital (now called Cedars-Sinai Medical Hospital) in Los Angeles, and Professor of Neurological Surgery at the University of Southern California School of Medicine. By 1957, Dr. Seletz had treated more than 20,000 injury patients, and he began publishing a series of articles pertaining to whiplash trauma and headaches. Three of his articles are reviewed below.
Craniocerebral Injuries and the Postconcussion Syndrome
Journal of the International College of Surgeons
January, 1957; 27(1):46-53
The perception of headache is as a consequence of an electrical signal being interpreted in the sensory homunculus of the brain. In this article, Dr. Seletz discusses the origin of the headache electrical signal using the neuroanatomical relationships between the 2nd cervical nerve root, the trigeminal nerve (cranial nerve V), and the spinal accessory nerve (cranial nerve XI).
Dr. Seletz notes that human corticospinal reflexes are inadequate to prevent injuries from motor vehicle collisions. Consequently, motor vehicles are “actually potentially lethal weapons, comparable to pearl-handled machine guns.” Every year they account for 40,000 deaths and 1,000,000 disablements in the United States.
Dr. Seletz notes that many patients involved in whiplash trauma will develop incapacitating severe headaches that may persist for months or even years. However, because the patient suffered no loss of consciousness, they are “neglected by the general practitioner and the specialist alike.” Consequently, the true etiology for the headache is often not thoroughly evaluated.
Often, these patients have normal examinations weeks after injury, but still complain of “severe headaches and exhaustion, as well as inability to return to normal [work] duties.” The headaches are often severe, begin in the suboccipital area and radiate to the vertex or to behind one eye; or they may be frontal or temporal. These persons are often accused of malingering or having litigation neurosis.
Dr. Seletz believes that the true cause of these headaches is extracranial in origin. Specifically he states:
“Analysis of the symptoms of several thousands of such patients will reveal that headaches persisting for months or years after a cerebral concussion are real and that they are extracranial in origin.”
The two primary extracranial sources for these headaches are:
1) The upper cervical spinal nerve roots.
2) Elements of the trigeminal nerve.
Alternatively, a combination of the two may exist. Dr. Seletz refers to the complex symptoms that follow injuries to the head and neck as the craniocervical syndrome.
Dr. Seletz notes that in every motor vehicle collision, the vehicle occupants “always undergo some degree of cervical sprain.” In every whiplash injury, the head is involved in sudden acceleration or deceleration, causing some unnatural movement, rotation or strain by the upper cervical spinal roots and muscles.
Dr. Seletz believes that the 2nd cervical nerve root is most often involved in the generation of headaches. He states:
“The 2nd cervical nerve root is more vulnerable to trauma than other nerve roots because it is not protected by pedicles and facets.”
Problems with the 2nd cervical nerve root include giddiness, unsteadiness, occasional nausea, and disturbances in focusing the eye. The 2nd cervical nerve root becomes the greater occipital nerve as it pierces the tendon of the trapezius muscle. It supplies the sensory innervation, including pain, to most of the scalp, the upper portion of the neck and portions of the face.
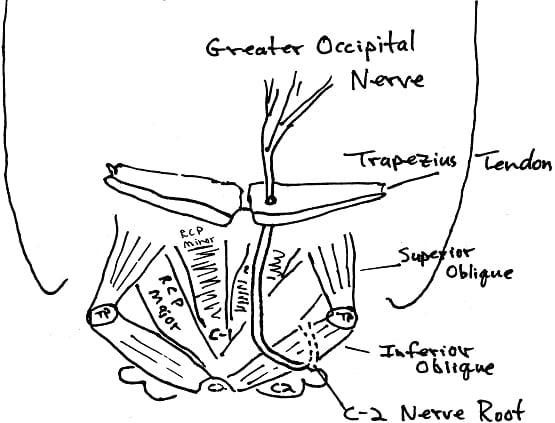
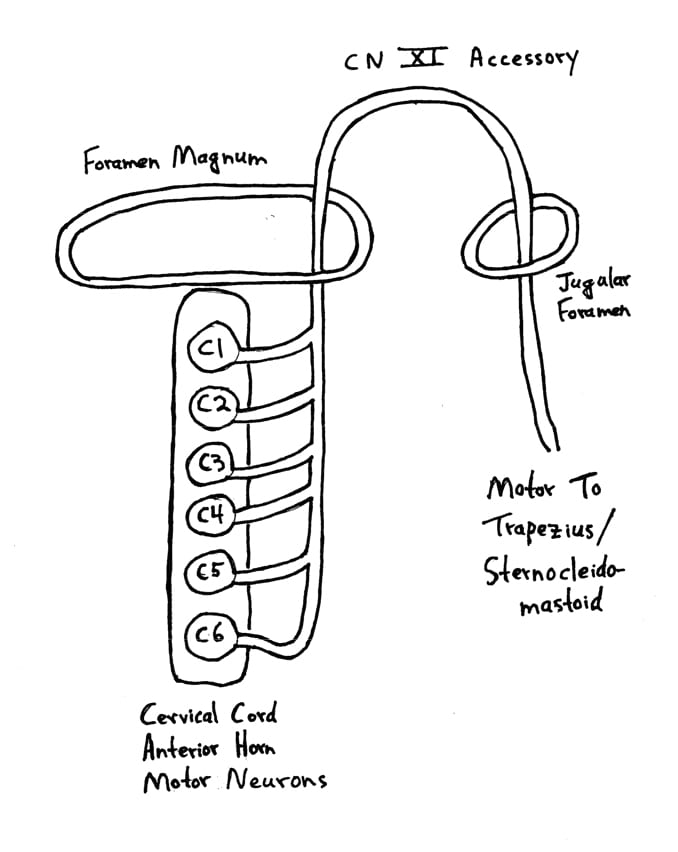
Dr. Seletz notes that the spinal accessory nerve takes its origin from the entire length of the cervical cord, “always as low as the fifth and often as low as the seventh cervical level.” Consequently, “any acute flexion, extension or torsion of the neck will exert traction on the delicate filaments [of origin] of the spinal accessory nerve, resulting in spasm of the trapezius and sternocleidomastoid muscles.”
When the trapezius and suboccipital muscles (especially the inferior oblique muscle) are in spasm, “traction is produced upon the greater occipital nerve as it pierces the fascial attachment of these muscles.” As shown, the 2nd cervical nerve root leaves the interspace between C1-C2, courses down and winds under the inferior oblique muscle, then proceeds upward as the greater occipital nerve, and pierces the tendon of the trapezius muscle.
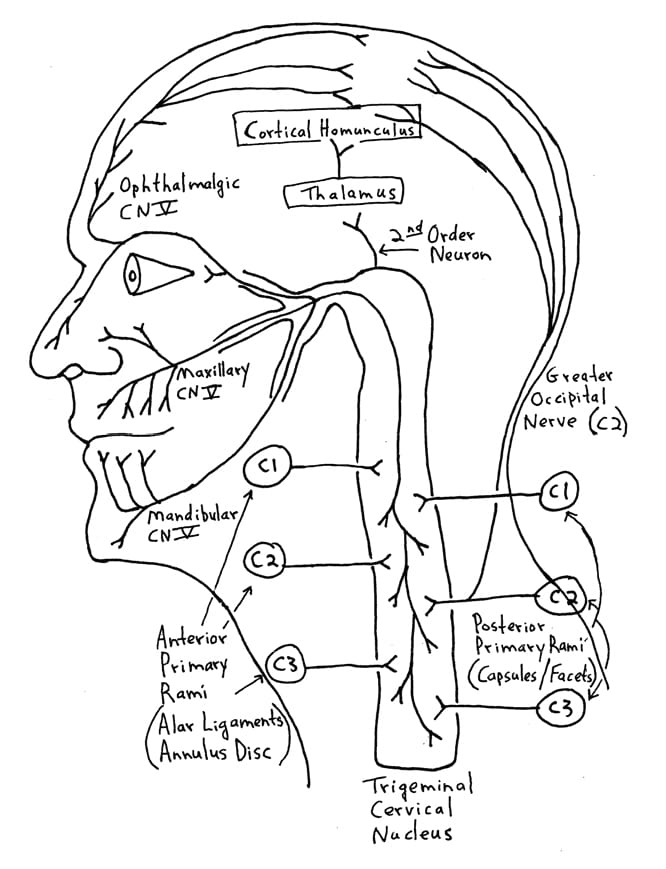
The three sensory branches (ophthalmic, maxillary, mandibular) of the trigeminal nerve (cranial nerve V) are shown above. Sensory changes, including headache, extending over the trigeminal innervation area following whiplash injury to the neck are explained by the communication between the 2nd and 3rd cervical nerve roots and the greater occipital nerve with the trigeminal nerve in the spinal fifth tract of the medulla. This has been called the greater occipital/trigeminus syndrome, and is a cause of post-whiplash headache.
The ophthalmic fibers of cranial nerve V descend the deepest into the cervical spine. Consequently, traumatized patients often perceive their headache in the distribution of the ophthalmic branch, around and behind the eye.
Dr. Seletz notes that inertial trauma to the head can occasionally result in direct trauma to the scalp (contusion), and that such scalp trauma may leave a superficial or subcutaneous scar. Because the scalp is innervated by sensory branches of the greater occipital nerve (C2) and/or branches of cranial nerve V, such scars may “give rise to bouts of severe and persistent headache.” Digital pressure on these minute palpable scars may “initiate the entire migraine-like syndrome.” Treatment is to the scar.
Although Dr. Seletz does not elaborate on treatment strategies in this article, he will do so in subsequent articles on the subject.
••••••••••
Dr. Seletz’s next pertinent article was published the following year:
Headache of Extracranial Origin
California Medicine
November 1958, Vol. 89, No. 5, pp. 314-17
In this article, Dr. Seletz continues to discuss the neuroanatomical relationships between the spinal accessory nerve (cranial nerve XI), the trapezius muscle, the greater occipital nerve, the C2 nerve root, and headaches. Additionally, he discusses the role of the vertebral arteries and their physiological relationship to the post-ganglionic sympathetic nerves.
Dr. Seletz notes that the cervical intervertebral foramina, although appearing roomy, are constricted by cartilage, by the vertebral artery, and by the lateral intervertebral joints, also known as the uncinate processes. Osteophytosis, swelling or adhesions in this constricted intervertebral foramina space almost inevitably causes painful vascular or neural disorder. Dr. Seletz states:
“Encroachment within the cervical foramina, irritating the nerve roots, may be due to occupational or disease deformity or to bony overgrowth, but most often it is due to trauma.”
Ruth “Jackson [MD] expressed belief that 90% of patients with symptoms of cervical nerve root irritation have had a sprain of the cervical spine at some time. Often the injury is minor and eventually forgotten.”
Three fourths of the cervical spine neural foramen is “occupied by structures other than the nerve root, [such as the vertebral artery and its adnexae] and additional space may be occupied by the rarely mentioned lateral intervertebral joint.”
The lateral intervertebral joints, mentioned above, are located at the lateral margins of the cervical disc as a “small synovial joint,” first described by Von Luschka in 1858. Other names for these joints of Von Luschka include:
Uncinate processes, Covertebral articulations, Uncovertebral joints, Neurocentral joints, and the Lateral intervertebral joints.
Dr. Seletz notes that where the nerve root emerges from the vertebra, it is in intimate contact with the lateral intervertebral joint, and is subject to potential irritation with every turn of the head. On degenerative thinning of the disc (especially after trauma) the processes of the lateral joints are gradually forced out laterally, causing spurs or osteophytes. These osteophytes can project laterally, encroaching upon the contents of the intervertebral foramen or foramen transversarium. Since these osteophytes have a radiotranslucent cartilage cap, the encroachment is always greater that that shown on a standard x-ray.
Dr. Seletz notes that another source of nerve root irritation is subsequent to neck sprain “in which hemorrhage into capsular ligaments of the lateral joints, no matter how minute, causes adhesions, between the ligaments and the dural sleeve of the nerve roots.” Dr. Seletz states:
“The author has observed, at operation, severe nerve root swelling and dural adhesions at this point, despite failure to demonstrate the abnormality by roentgenography and electromyography.”
Pertaining to the vertebral arteries, Dr. Seletz reviews the syndrome of of Barre-Lieou, which was first described in 1925-1928. The syndrome of Barre-Lieou consists of migraine-like symptoms attributed to disturbance of sympathetic tone about the vertebral artery. Typical symptoms include severe headache, cervical pain, tension headache and occasionally facial neuralgia. There are also reports of diplopia, ataxia, and disturbance in swallowing.
In certain postures of the neck the vertebral artery is constricted or even occluded. Traction or sprain may likewise cause headache through disturbance of the vertebral arterial [sympathetic] nerves, the posterior cervical autonomic system or the spinal accessory nerves which originate in delicate filaments from all points of the cervical spinal cord.
It is documented that Barre-Lieou syndrome can be caused by sprain of the cervical spine. Dr. Seletz states:
“The vertebral [sympathetic] nerve originates from the stellate [inferior cervical sympathetic] ganglion and ascends in the transverse foramen, along with the vertebral artery. It supplies the vertebral and basilar arteries—the major blood supply to the pons and medulla, including the area that contains the nuclei of origin of the 5th, 6th, 7th, 8th, 9th, 10th 11th cranial nerves.”
Pertaining to the spinal accessory nerve (cranial nerve XI), Dr. Seletz notes that it originates from many filaments from the entire length of the cervical spinal cord. Dr. Seletz states:
“Any acute torsion, flexion, extension or rotation of the neck exerts traction on these delicate filaments, resulting in spasm of the trapezius and sternomastoid muscles.”
Such spasm of the trapezius muscle exerts traction on the greater occipital nerve at the point of where the nerve pierces the tendinous attachment of the upper trapezius muscle, resulting in occipital pain and headache. The greater occipital nerve innervates the scalp, the upper part of the neck and portions of the face. The C2 nerve root becomes the greater occipital nerve as it pierces the tendon of the trapezius at the base of the skull.
Additionally, the C2 nerve root is the most vulnerable to trauma because “it is not protected posteriorly by pedicles and facets.” Cervical trauma causes a “tractional injury” to the C2 nerve root because its exit is between C1 and C2, the point of “greatest rotation of the head on the neck.”
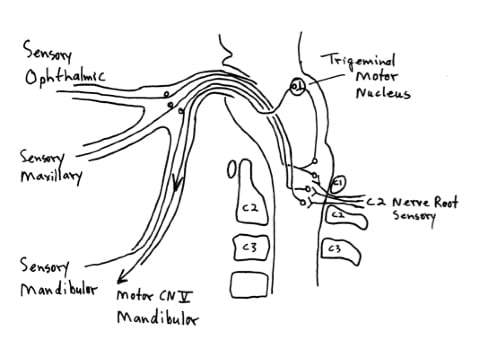
There is a communication between the sensory fibers of the greater occipital nerve (C2 nerve root) and the first division (ophthalmic) in the spinal 5th tract of the medulla [trigeminal cervical nucleus]. This gives rise to pain behind the eye. “The patient often feels as if the eyeball is being torn from the socket. The headaches are migraine-like and often associated with nausea, vomiting and blurred vision.” The migraine-like suboccipital and retro-orbital headache is due to disturbance of the second cervical nerve, which communicates with the first division of the trigeminal nerve.
This is the mechanism by which neck sprain can cause hemicrania.
Lastly, Dr. Seletz once again notes that an old scalp contusions [scar tissue] can cause persistent, recurrent, severe headaches. This mechanism of extracranial headache is often overlooked.
••••••••••
The last article I reviewed by Dr. Emil Seletz was published in the Journal of the American Medical Association:
Whiplash Injuries
Neurophysiological Basis for Pain and Methods Used for Rehabilitation
Journal of the American Medical Association
November 29, 1958, pp. 1750 – 1755
In this article, Dr. Seletz continues to review similar neuroanatomical relationships, pathoanatomy, and pathophysiology that can cause headaches. Additionally, he elaborates on pertinent clinical protocols to help successfully treat these extracranial sources of headache. Dr. Seletz states:
“Direct trauma results to the spinal accessory nerve and to the roots of the cervical nerves, but in addition there are vasomotor disturbances resulting indirectly from damage to the vertebral arteries and to nerve fibers that accompany these arteries in their course through the foramina transversaria.”
“The disabling and persistent symptomatology in the vast majority of [whiplash] cases is due to involvement of the delicate and vital nerves and blood vessels about the cervical spine.”
“The origin of the pain and disturbed function lies in the involvement of various cervical roots, the spinal accessory nerve and the cervical autonomic nerve, including the vertebral [sympathetic] nerve, and in the transient obstruction or compression of the vertebral artery.”
Once again Dr. Seletz emphasizes the importance of the C2 nerve root. A major portion of the headaches associated with the whiplash syndrome are derived from a traction injury to the second cervical nerve root. The second cervical nerve root is particularly vulnerable to injury because it is not protected by pedicles and facets, as are the other cervical nerve roots. Also, the second cervical nerve root exits between the atlas and axis, “the point of greatest rotation of the head on the neck.”
“The physiological communication between the second cervical and the trigeminal nerves in the spinal fifth tract of the medulla [trigeminal-cervical nucleus] involves the first division of the trigeminal nerve [ophthalmic] and thereby gives attacks of hemicrania with pain radiating behind the corresponding eye.” Since the greater occipital nerve pierces the tendonous attachment of the trapezius muscle at the base of the skull, trapezius spasm aggravates greater occipital nerve (C2) sensory disturbance. This is the mechanism whereby a great many chronic and persistent headaches have their true origin in injury to the second cervical nerve, noting:
“Many headaches are not headaches at all, but really a pain in the neck.”
Pertaining to the vertebral artery, Dr. Seletz notes”
“The vertebral nerve lies within the transverse foramina and travels alongside the vertebral artery. The vertebral nerve originates from the stellate ganglion [inferior cervical sympathetic ganglion] and supplies the vertebral and basilar vessels. Injury to this nerve produces spasm of the vertebral arteries and gives rise to disturbed circulation to the pons and portions of the medulla containing the nuclei of origin of the lower seven cranial nerves, with resultant far-flung symptoms.”
“Very little slack exists in the vertebral artery and, during severe hyperextension and hyperflexion and especially during extreme lateral rotation, partial to complete obstruction of the vertebral artery has been demonstrated by arteriography.”
Angiography has shown constriction or occlusion of the vertebral artery in patients with persistent symptoms of vertigo, ataxia, headache, diplopia, and unsteadiness of gait. “The usual site of occlusion is at the second cervical level, which is the point of greatest rotation of the head on the neck.”
“A great majority of symptoms that have been designated as psychoneurotic, namely, attacks of vertigo, ataxia, diplopia, severe attacks of migraine-like headache, hemicrania with nausea and vomiting, and, at times disturbances of speech and swallowing, are all due to disturbed circulation of the vertebral artery after neck sprain.”
As noted, in this article, Dr. Seletz elaborates on treatment. He states:
“If the blood vessel wall has been traumatized during the injury or the vertebral nerve [sympathetic] has been injured, vasospasm persists. The only true, effective measures for tiding over this stage of injury lie in adequate physical therapy.”
“Treatment must be started early and must be administered by those expertly trained in physical therapy and rehabilitation.”
“Those patients not receiving adequate therapy will not improve and will soon become discouraged and resentful.”
“In reviewing the types of treatment with a number of specialists in this field, it is found that, while therapy naturally varies to suit the individual need, it consists primarily of local heat in the form of hot wet packs and cervical traction, followed by very gentile massage and manual rotations.”
“Local hot packs relieve the muscle spasm, increase the blood flow, and frequently stop severe occipital pain and headaches.”
“During injury, hemorrhage within the capsular ligaments gives rise to swelling of the nerves and eventually adhesions between the dural sleeve and the nerve root; these factors give rise to symptoms that may be prolonged for months or even years after the injury.”
“The importance of a carefully planned scheme of treatment must be emphasized to the patient, and treatments must be religiously carried out daily during the first two or three weeks (and then about three times weekly), depending, of course, on the individual case.”
“Delay or faulty treatment leads to adhesions about the facets and scarring about the capsular ligaments, persistent spasm, congestive lymph edema, and fibrosis of muscles, swelling, and eventual adhesions of nerves within the nerve root canals.”
“The resultant faulty posture in neglected cases enhances the degeneration of the intervertebral disks, as well as spur formation in the lateral co-vertebral articulations, which on the roentgenogram has come to be known as traumatic arthritis.”
“I cannot too strongly emphasize the urgency of early and persistent therapy, always by a specialist in this field.”
“I wish to emphasize the importance of traction in helping to relieve obstruction to the course of the vertebral arteries.”
“Early and adequate traction may prevent the formation of adhesions between the dural sleeve of the nerve roots and the adjacent structures.”
“Occasionally, a patient is seen with persistent complaints of head, neck, and shoulder pain, who has had on surgical exposure persistent swelling and adhesions of several nerve roots within the dural sleeve of exit. It is most likely that early, persistent, and adequate therapy by those expertly trained in physical medicine will prevent most patients from developing a surgical condition.”
“The procedure outlined here includes heat, manipulation, and traction.”
“Carefully adapted to the individual case, this plan generally obviates the danger of surgical and psychiatric complications.”
SUMMARY
Today’s chiropractor is well educated in the concepts reviewed above by Dr. Emil Seletz. They have an in depth understanding of the neuroanatomical relationships between the cervical spine and the perception of headache. In addition, they are extremely sensitive to the importance of the vertebral artery and the potential for mechanical treatments to influence the vertebral artery. Chiropractors are true experts in the field of rehabilitation of cervical spine disorders, including the protocols emphasized by Dr. Seletz: manual rotations, manipulations, heat, massage, traction, and exercise.
